


 Sign Out
Sign Out
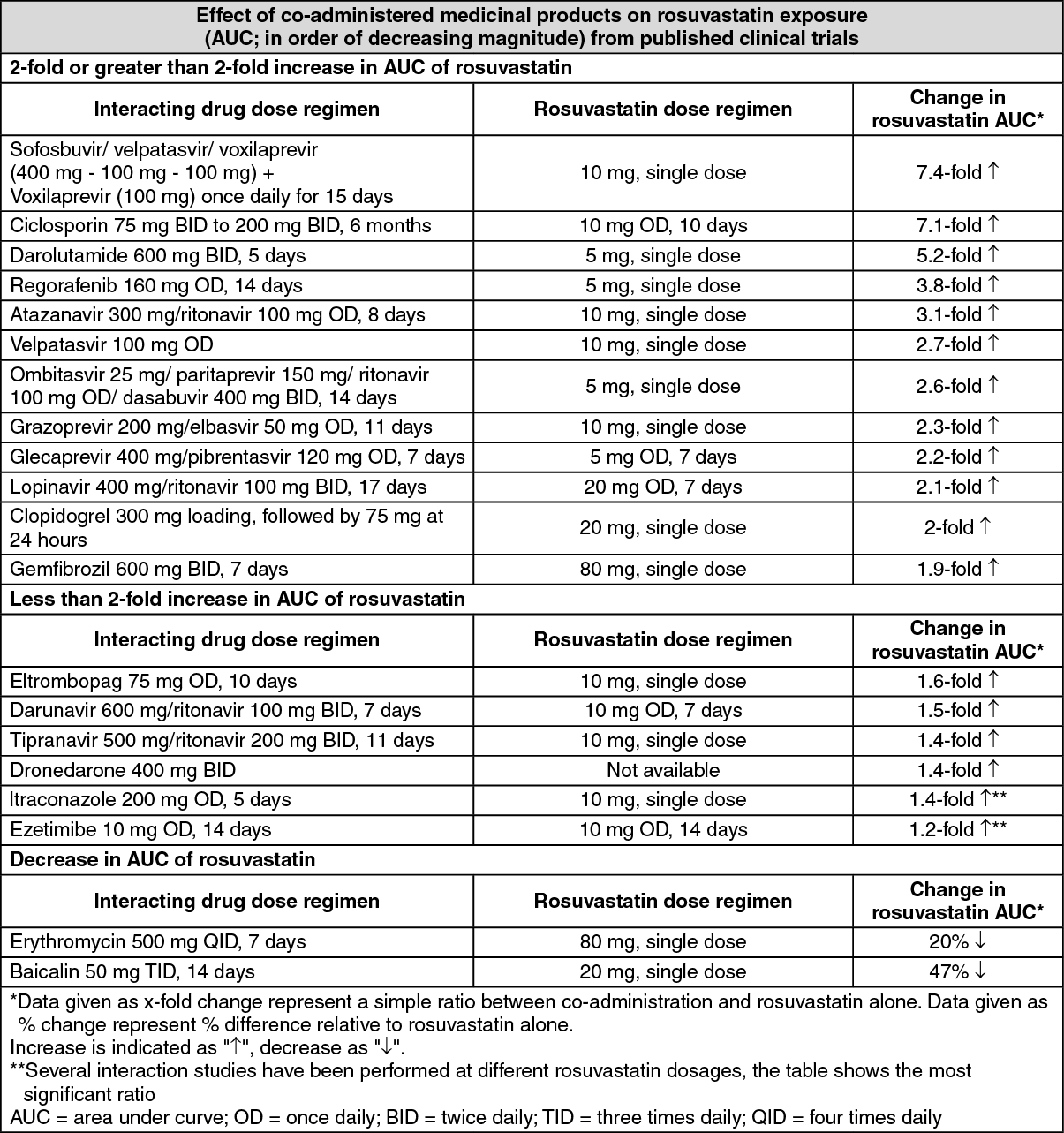
Ciclosporin: During concomitant treatment with rosuvastatin and ciclosporin, rosuvastatin AUC values were on average 7 times higher than those observed in healthy volunteers. Rosuvastatin is contraindicated in patients receiving concomitant ciclosporin. Concomitant administration did not affect plasma concentrations of ciclosporin.
Protease inhibitors: Although the exact mechanism of interaction is unknown, concomitant protease inhibitor use may strongly increase rosuvastatin exposure (see table). For instance, in a pharmacokinetic study, co-administration of 10 mg rosuvastatin and a combination product of two protease inhibitors (300 mg atazanavir / 100 mg ritonavir) in healthy volunteers was associated with an approximately three-fold and seven-fold increase in rosuvastatin steady-state AUC and Cmax respectively. The concomitant use of rosuvastatin and some protease inhibitor combinations may be considered after careful consideration of rosuvastatin dose adjustments based on the expected increase in rosuvastatin exposure.
Gemfibrozil and other lipid-lowering products: Concomitant use of rosuvastatin and gemfibrozil resulted in a 2-fold increase in rosuvastatin Cmax and AUC.
Based on data from specific interaction studies no pharmacokinetic relevant interaction with fenofibrate is expected, however a pharmacodynamic interaction may occur. Gemfibrozil, fenofibrate, other fibrates and lipid lowering doses (> or equal to 1 g/day) of niacin (nicotinic acid) increase the risk of myopathy when given concomitantly with HMG-CoA reductase inhibitors, probably because they can produce myopathy when given alone. The 40 mg dose is contraindicated with concomitant use of a fibrate. These patients should also start with the 5 mg dose.
Ezetimibe: Concomitant use of 10 mg rosuvastatin and 10 mg ezetimibe resulted in a 1.2-fold increase in AUC of rosuvastatin in hypercholesterolaemic subjects (see table). However, a pharmacodynamic interaction, in terms of adverse effects, between rosuvastatin and ezetimibe cannot be ruled out.
Antacid: The simultaneous dosing of rosuvastatin with an antacid suspension containing aluminium and magnesium hydroxide resulted in a decrease in rosuvastatin plasma concentration of approximately 50%. This effect was mitigated when the antacid was dosed 2 hours after rosuvastatin. The clinical relevance of this interaction has not been studied.
Erythromycin: Concomitant use of rosuvastatin and erythromycin resulted in a 20% decrease in AUC and a 30% decrease in Cmax of rosuvastatin. This interaction may be caused by the increase in gut motility caused by erythromycin.
Cytochrome P450 enzymes: Results from in vitro and in vivo studies show that rosuvastatin is neither an inhibitor nor an inducer of cytochrome P450 isoenzymes. In addition, rosuvastatin is a poor substrate for these isoenzymes. Therefore, drug interactions resulting from cytochrome P450-mediated metabolism are not expected. No clinically relevant interactions have been observed between rosuvastatin and either fluconazole (an inhibitor of CYP2C9 and CYP3A4) or ketoconazole (an inhibitor of CYP2A6 and CYP3A4).
Interactions requiring rosuvastatin dose adjustments (see table): When it is necessary to co-administer rosuvastatin with other medicinal products known to increase exposure to rosuvastatin, doses of rosuvastatin should be adjusted. Start with a 5 mg once daily dose of rosuvastatin if the expected increase in exposure (AUC) is approximately 2-fold or higher. The maximum daily dose of rosuvastatin should be adjusted so that the expected rosuvastatin exposure would not likely exceed that of a 40 mg daily dose of rosuvastatin taken without interacting medicinal products, for example a 20 mg dose of rosuvastatin with gemfibrozil (1.9-fold increase), and a 10 mg dose of rosuvastatin with combination ritonavir/atazanavir (3.1-fold increase). If medicinal product is observed to increase rosuvastatin AUC less than 2-fold, the starting dose need not be decreased but caution should be taken if increasing the rosuvastatin dose above 20 mg. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe following medical product/combinations did not have a clinically significant effect on the AUC ratio of rosuvastatin at co-administration: Aleglitazar 0.3 mg 7 days dosing; Fenofibrate 67 mg 7 days TID dosing; Fluconazole 200 mg 11 days OD dosing; Fosamprenavir 700 mg/ritonavir 100 mg 8 days BID dosing; Ketoconazole 200 mg 7 days BID dosing; Rifampin 450 mg 7 days OD dosing; Silymarin 140 mg 5 days TID dosing.
Effect of rosuvastatin on co-administered medicinal products: Vitamin K antagonists: As with other HMG-CoA reductase inhibitors, the initiation of treatment or dosage up-titration of rosuvastatin in patients treated concomitantly with vitamin K antagonists (e.g. warfarin or another coumarin anticoagulant) may result in an increase in International Normalised Ratio (INR). Discontinuation or down-titration of rosuvastatin may result in a decrease in INR. In such situations, appropriate monitoring of INR is desirable.
Oral contraceptive/hormone replacement therapy (HRT): Concomitant use of rosuvastatin and an oral contraceptive resulted in an increase in ethinyl estradiol and norgestrel AUC of 26% and 34%, respectively. These increased plasma levels should be considered when selecting oral contraceptive doses. There are no pharmacokinetic data available in subjects taking concomitant rosuvastatin and HRT and therefore a similar effect cannot be excluded. However, the combination has been extensively used in women in clinical trials and was well tolerated.
Other medicinal products: Digoxin: Based on data from specific interaction studies no clinically relevant interaction with digoxin is expected.
Fusidic acid: The risk of myopathy including rhabdomyolysis may be increased by the concomitant administration of systemic fusidic acid with statins. The mechanism of this interaction (whether it is pharmacodynamic or pharmacokinetic, or both) is yet unknown. There have been reports of rhabdomyolysis (including some fatalities) in patients receiving this combination. If treatment with systemic fusidic acid is necessary, rosuvastatin treatment should be discontinued throughout the duration of the fusidic acid treatment.
Paediatric population: Interaction studies have only been performed in adults. The extent of interactions in the paediatric population is not known.